

Craniofacial
Appearance In Individuals with Emanuel Syndrome
Some children with Emanuel Syndrome, as mentioned previously, appear to resemble each other, and often are labelled by medical professionals as being “dysmorphic” which is basically defined as someone having an atypical appearance.
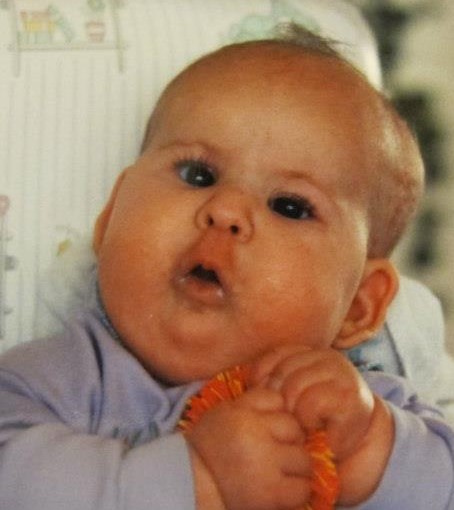
Some of our children have deep-set eyes, lower-set ears, and a longer upper lip (referred to as “philtrum”) which you can see clearly here when Maia was a baby.
Some features seen in the faces of people with ES may include:
- Hooded eyelids
- Ptosis (drooping upper eyelids)
- Deep-set eyes
- Upslanting palpebral fissures (the opening between the eyelids)
- Low hanging columnella (the bridge of tissue that separates the nostrils at the nasal base)
- Micrognathia (a smaller than typical jaw – see below)
- Facial asymmetry/Hemifacial microsomia (see below)
Cleft palate

A cleft palate is an incomplete closure of the roof of the mouth during the development of the fetus. Cleft palate is sometimes seen in conjunction with Pierre Robin Sequence, a combination of cleft palate, small jaw (micrognathia) and a downward, displacement of the tongue (which is further back in the airway than normal, and referred to as glossoptosis.) Cleft palate is seen in approximately 50% of children with Emanuel syndrome. It can be full, affecting both the hard and soft palate, or just the soft palate. This is a picture of Maia, who had a complete cleft palate. You can see in the photo she is missing the palate.
A cleft palate is an incomplete closure of the palate (the boney part at the top of your mouth) and/ or the soft palate (the soft part at the back of the mouth) and uvula (the ‘dangly bit’ at the back of the mouth.
See John Hopkins All Children’s Hospital for information on Pierre Robin sequence.
Cleft palates can lead to problems with feeding and, if combined in Pierre Robin Sequence, difficulties with breathing as well. Cleft palates are repairable with surgery, which usually takes place around 1 year of age. Some of our children have less serious forms of clefting, seen as submucous clefts, or bifid uvulas (where the uvula – located at the back of the throat – appears to be split in two.) Some children may have very high arched palates. Cleft lip is not typically seen, but has been reported by Luo 2017.
Micrognathia
Micrognathia (a smaller than normal jaw) is very common and can be seen as part of Pierre Robin sequence. Some children with Emanuel Syndrome in our group have undergone treatments called jaw distraction surgery (Mandibular Distraction Osteogenesis (MDO) ) to improve the symptoms associated with having a very small jaw.

Maia – note the recessed jaw
See Seattle Children’s Hospital website for information about distraction surgery.
Skull Differences / Facial Asymmetry / Cranial Microsomia – Differences in size and shape on the left and right sides of the skull (see https://medlineplus.gov/genetics/condition/craniofacial-microsomia/)
Other less common appearance findings can include:
- High arched palate
- Facial palsy
- Uvular hypoplasia / Bifid uvula

“Kieren was diagnosed late with both plagiocephaly and brachycephaly. Due to this, wearing two cranial reshaping braces/helmets only provided minimal repairs. Having testosterone shots may have also jumpstarted the plates closing. But the main goal of having his eyes come back into alignment was reached. As always, Kieren met this with sass and fierce objection.”
Additional supports
Wide Smiles: https://widesmiles.org/
About Face https://www.aboutface.ca/
American Cleft Palate – Craniofacial Association https://acpa-cpf.org/
Craniostenosis – Plagiocephaly support page (CAPPSKIDS)
Book recommendation
Children with Cleft Lip and Palate: A Parents’ Guide to Early Speech-Language Development and Treatment
References
Carter, M. T., St Pierre, S. A., Zackai, E. H., Emanuel, B. S., & Boycott, K. M. (2009). Phenotypic delineation of Emanuel syndrome (supernumerary derivative 22 syndrome): Clinical features of 63 individuals. American Journal of Medical Genetics. Part A, 149A(8), 1712–1721. https://doi.org/10.1002/ajmg.a.32957
You may also be interested in: Emanuel Syndrome Development